I’ve been reading lately about the various forces we as implant surgeons need to consider. I’ll admit this is an aspect of learning about dental implants that can be a little dry. In fact the words, “finite element analysis” put me instantly to sleep 9 times out of 10. So in order to save you some time, I wanted to list some high yield concepts about masticatory forces and how they affect dental implant success and longevity.
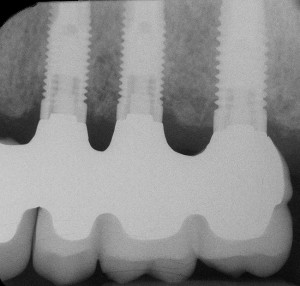
The first consideration is that forces applied to a natural tooth are distributed more or less evenly throughout the periodontal ligament. This is not so with an implant. Because an implant is meant to be in direct bone contact, the result is that forces applied to an implant are concentrated in the crestal bone surrounding the implant and are less present near the implant apex.
Failing to consider the forces that will be placed upon every implant you place can lead to the following complications: implant or component fractures, crestal bone loss, porcelain fracture, abutment screw loosening, or even total implant loss. So…..consider the following:
- Average biting forces range from 20-350lbs with the molar region being subject to greater forces (200+), the canine region being subject to less (100+), and the incisors being subject the least (25-40). (Scott I, Ash MM Jr: A six channel intra-oral transmitter for measuring occlusal forces, J Prosthetic Dentistry 16:56, 1966)
- Parafunctional forces can reach near 1000lbs. (Graf H: Bruxism, Dental Clinics of North America 13:659-665, 1969)
- Natural teeth come in to contact during eating and swallowing. Normally this would amount to 30 minutes of contact per day. (Graf H: Bruxism, Dental Clinics of North America 13:659-665, 1969)
- Fatigue fractures in implants and their components are related to the forces they sustain and the number of times they are loaded over time.
- Bone can best resist compressive forces. It is weaker by about 30% when resisting tension, and weaker by 65% under shearing forces. (Misch, CE, et al: Bone density: effect on treatment planning…., International Journal of Oral Implantology 6:23-31, 1990) (Misch, et al: Mechanical properties of trabecular bone in the human mandible: implications for dental treatment planning…., Journal of Oral & Maxillofacial Surgery 57:700-706, 1999)
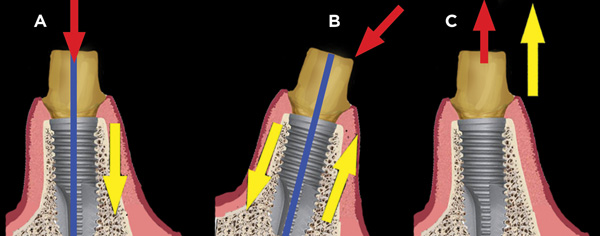
- Implants are best placed with an orientation perpendicular to the curves of Spee and Wilson. Small increases in angled loads result in increases in lateral shear forces on the implant and therefore bone, and bone is weakest at resisting shear forces.
- Bone density is directly related to bone strength. Alveolar bone that has been edentulous undergoes a loss of bone density. This is most prevalent in the posterior regions.
- An implant placed in dense bone transfers a majority of occlusal force to the first 5mm of crestal bone. (Rieger MR, et al: Finite element analysis of bone-adapted and bone-bonded endosseous implants, Journal of Prosthetic Dentistry 62: 436-440)
These concepts should help with your planning which should proceed from the prosthesis to the anticipated forces the implant must sustain, and ultimately to the implant size selection.
In cases where conditions are not ideal, choose wider or longer implants, or consider appropriate occlusal schemes to protect the implant from excessive forces. Doing this will give the best chances for long term success.